
Ask the billing manager at most orthopedic ASCs what their denial rate is, and you'll get a number. Ask them what their denial rate is for total knee arthroplasty versus total hip replacement, or broken out by payer, and the answer is usually a pause.
That gap in visibility is part of why ASC denial rates for ortho procedures routinely run 2-3x higher than the same procedures performed at a hospital — and why most facilities don't realize how much the disparity is costing them.
This is not an operational failure. It's a structural one. The reasons ASC denial rates run higher are baked into how payers have designed their reimbursement rules for facility settings. Understanding the mechanics is the first step to managing them.
The Benchmark Gap
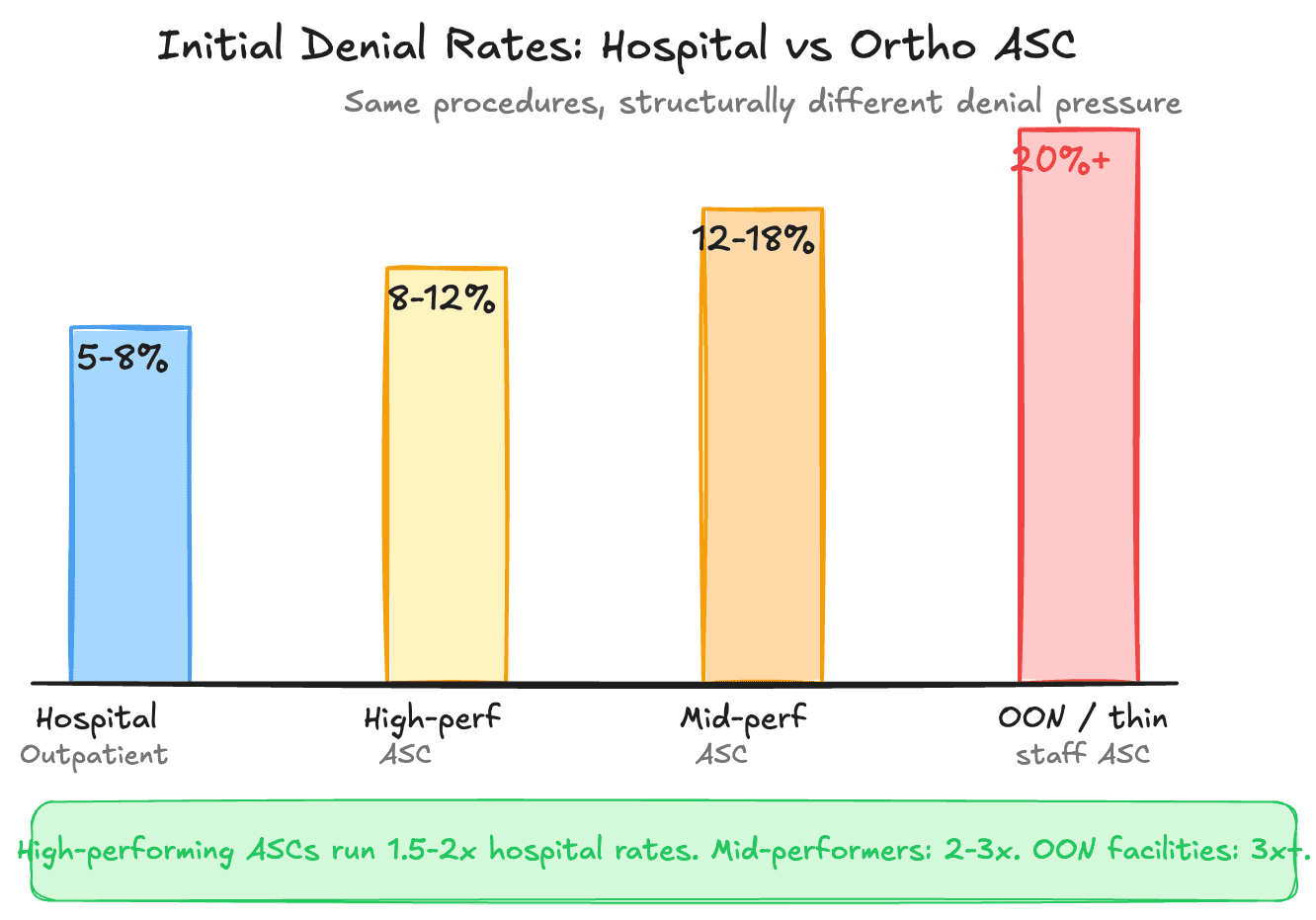
Industry benchmarks vary, but the pattern is consistent. Hospitals with dedicated revenue cycle departments see initial denial rates in the 5-8% range across their case mix. High-performing ortho ASCs — the ones with experienced billing staff and solid workflows — can hit 8-12%. Mid-performing ASCs see 12-18%. For ASCs with OON exposure or thin staffing, initial denial rates above 20% are not unusual.
The comparison is imperfect because hospitals and ASCs bill differently. But when the same procedure — a total knee replacement, for example — is billed by a hospital-based outpatient department versus an independent ASC, the denial rate differential is real and documented. CMS facility billing data, MGMA benchmark surveys, and HFMA studies all point in the same direction: independent ASCs face structurally higher denial pressure for ortho cases.
Three factors drive the gap. Each one compounds the others.
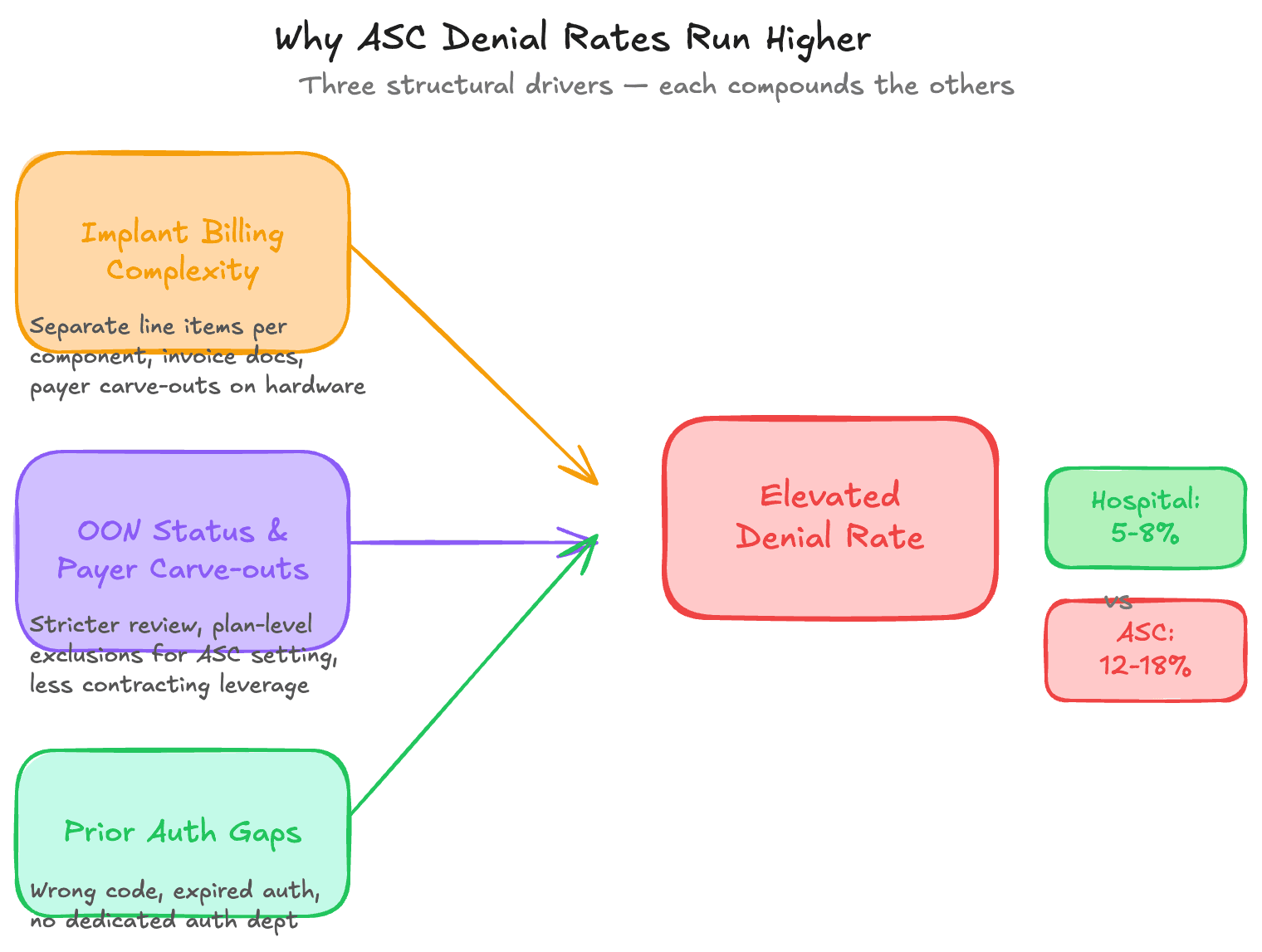
Implant Billing: The Highest-Surface Denial Driver
Orthopedic surgery is implant-intensive. A total knee replacement involves a femoral component, a tibial component, a tibial insert, and often a patellar component. Spine procedures involve cages, screws, and rods. Shoulder arthroplasties have their own hardware taxonomy. For many ortho procedures, the implant cost exceeds the facility fee.
Hospitals typically operate under negotiated all-inclusive or DRG-based rates that bundle implant costs into overall reimbursement. The billing complexity of the hardware disappears inside a single payment line.
ASCs don't have that option. They bill implants separately — and that's where the denial surface expands significantly.
Payers have specific, often inconsistently applied, policies for implant reimbursement. Some require invoice-based documentation and reimburse at cost plus a markup percentage. Others reimburse against an internal fee schedule that may not reflect actual acquisition cost. Some have carve-out policies that explicitly exclude certain implant categories from ASC coverage entirely.
Common implant denial triggers at ortho ASCs:
- Missing or misformatted invoice documentation. Payer policy requires the actual manufacturer invoice attached to the claim or submitted via portal, and it wasn't.
- Implant cost exceeds the "usual and customary" threshold. The payer caps reimbursement at a benchmark that doesn't reflect current hardware pricing.
- Wrong HCPCS code for the device. The L-code and C-code space for surgical supplies has gaps, and mismatches between what was used and what was billed trigger automatic denial.
- Payer carve-out for the specific device category. Some payers have quietly stopped covering certain implant types at the ASC level, requiring the case to be performed at a hospital outpatient department.
For a detailed look at how implant billing complexity translates into measurable write-offs, see our breakdown of implant billing revenue leakage in ortho ASCs.
OON Exposure and Payer Carve-Outs
The second structural driver is payer network status. Hospitals — especially large health systems — have contracting leverage. Payers need them in network. Most major regional and national payers have contracts with the dominant hospital in a market.
Independent ASCs have significantly less leverage. A newly opened ortho ASC, or a physician-owned ASC that hasn't prioritized contracting, may be OON with one or more major payers in its patient population.
OON status doesn't just mean lower reimbursement. It means a categorically different claims review process, higher scrutiny, and denial rates that are structurally elevated even for otherwise clean claims. Payers have more latitude to apply medical necessity criteria, documentation requirements, and timely filing rules more strictly for OON facilities.
Even for in-network ASCs, payer carve-outs create similar problems. A carve-out means a payer has excluded specific procedure categories from ASC coverage. Total joint replacement is the most common example. Many payers added ASC coverage for total knees and hips only after CMS expanded the inpatient-only exclusion list in 2020-2022, and some commercial payers still require hospital outpatient setting for these procedures for specific member populations.
An ASC that performs a total hip replacement on a member under a plan that carves out that procedure at the ASC level will receive a denial regardless of how clean the claim is. If denial codes aren't tracked systematically by payer and procedure, the same error repeats.
This is a specific variant of the broader ASC network isolation and OON exposure problem that affects independent facilities across specialties.
Prior Authorization as a Denial Multiplier
Ortho procedures are among the most prior-authorization-intensive in American medicine. Total joints, spine surgery, rotator cuff repairs, and most reconstructive procedures require pre-authorization from virtually every commercial payer. The requirements vary by payer, by plan type, by procedure code, and sometimes by individual surgeon.
Hospitals have dedicated prior auth departments. Large health systems have real-time eligibility and authorization verification integrated into scheduling and registration workflows. When a patient arrives for surgery at a hospital, someone has already confirmed the auth is in place and matches what's being performed.
At an independent ASC, this function often sits with one or two billing staff members who are also handling coding, charge entry, and claim follow-up. Authorization verification is a step in a sequence, not a dedicated function.
The denial patterns that result are predictable. Authorization was obtained for the wrong procedure code. The authorization expired before the surgery date. The auth was for one plan but the patient was covered under a different plan at time of service. The procedure differed from the authorized procedure due to intraoperative findings, and a concurrent review wasn't obtained.
Each represents an avoidable denial — but only if the workflow catches it before the claim is submitted. For ASCs running manual auth tracking in spreadsheets, the error rate on complex ortho cases is structurally higher than at facilities with integrated workflows. Our breakdown of prior authorization denial management covers the most common failure patterns and what systematic tracking looks like.
The Blindspot: Not Knowing Denial Rate by Code
Here's what makes the above dynamics particularly expensive: most ASC operators manage against a single top-line denial rate. Total claims. Total denials. Denial percentage.
That number is useful for reporting. It is nearly useless for operations.
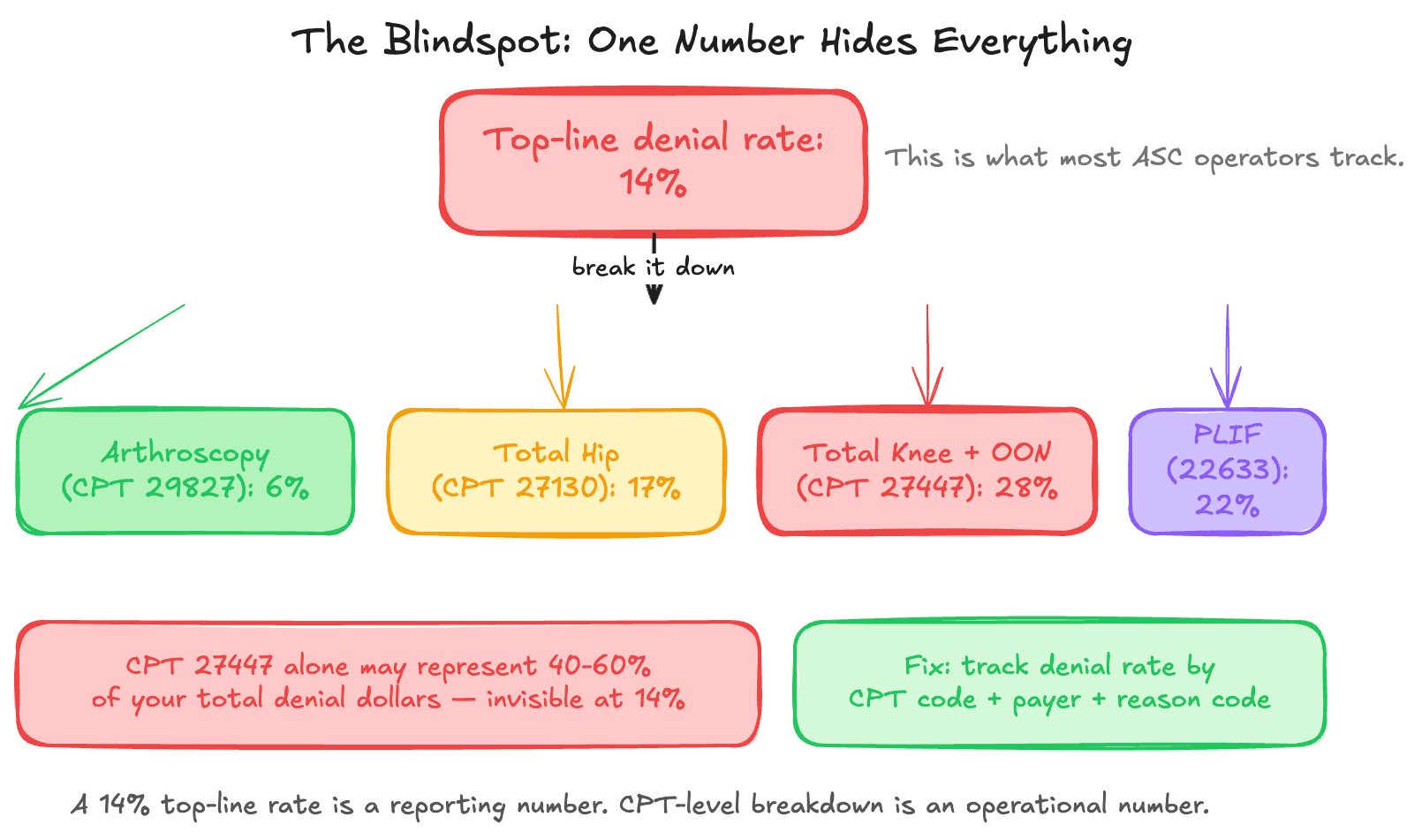
A 14% top-line denial rate could mean 5% on straightforward arthroscopy cases and 28% on total joint replacements with OON implant billing. It could mean one payer is responsible for 60% of total denials. It could mean prior auth failures on a specific CPT code cluster are generating the majority of write-off risk.
Without denial rate broken down by procedure code, payer, and denial reason code, the billing team is managing against an average that obscures every actionable signal.
This is the data visibility problem that precedes every operational fix. An ASC that doesn't know which procedures are generating the most denials cannot prioritize its intervention. Staff chase the loudest individual denials, not the most recoverable patterns.
The CPT codes most commonly associated with elevated denial rates in ortho ASCs:
- 27447 (Total knee arthroplasty) — implant billing complexity plus OON exposure plus auth stringency
- 27130 (Total hip arthroplasty) — payer carve-outs for ASC setting plus implant billing
- 29827 (Arthroscopic rotator cuff repair) — medical necessity documentation requirements
- 22633 (Posterior lumbar interbody fusion) — implant billing plus auth plus site-of-service disputes
- 27447 with modifier 22 (Increased procedural complexity) — medical necessity documentation for the add-on charge
An ASC running 200 ortho cases per month that doesn't know its denial rate by these codes is operating blind on the procedures that carry the highest reimbursement and the highest denial risk simultaneously.
What to Watch For
A few signals that suggest the structural gap is actively costing your facility:
- Implant claims are consistently under-reimbursed or denied without a clear payer response
- Authorization denials appear on procedures that were authorized — indicating a code mismatch or expiration issue
- One or two payers are responsible for a disproportionate share of your denial volume but you can't see this without manually pulling claims by payer
- Your denial rate is higher on new or higher-acuity procedures than on routine cases, but you're not tracking them separately
What This Means Operationally
The ASC denial rate gap versus hospitals is not a billing quality problem that can be fixed with additional training. It's a structural problem rooted in how payers have designed reimbursement rules for facility settings — and it requires structural responses.
That means tracking denial reason codes at the procedure-code level, not just rolling up to a facility total. It means payer-specific authorization verification workflows matched to each payer's actual requirements. It means implant billing documentation processes built around what each payer requires before the claim is submitted, not a generic invoice submission process.
Most ASCs are not running this level of operational detail because the manual overhead is prohibitive. The billing manager who is also handling coding and authorization verification does not have bandwidth to build a denial analytics function on top of daily workload.
The gap is real, the data is available, and the procedures generating it are identifiable. The question for most ortho ASC operators is whether they have the visibility to see it.
If your top-line denial rate looks acceptable but you've never broken it out by procedure code or payer, that's the place to start.